Anal Fissure
An anal fissure is a linear ulcer in the lower half of the anal canal and extends from just below the dentate line to the margin of the anus (anal verge). The ulcer may be acute, recurrent or chronic and may occur alone or with other rectal disease, most commonly hemorrhoids. An anal fissure is one of the chief causes of anal pain; in the acute case it is severe enough to incapacitate the patient. In fact it is a disease of the anus which causes an amount of suffering out of proportion to the size of the lesion. It is common in both the sexes and is encountered in young or middle aged adults, but is sometimes seen at other ages including infancy and early childhood.
Etiology
Trauma to the anal canal is the most common initiating factors usually in the form of passage of a large hard fecal mass.
Among the predisposing factors are –
- Inflammatory bowel disease.
- Previous anal surgery particularly haemorrhoidectomy.
- Anterior fissure develops in women due to child birth trauma.
- Persons taking laxatives or saline purgatives for a long period develops a degree of anal stenosis which may predispose to fissure formation, such patients have had only liquid motions for months or years and their anal canal has undergone some degree of contraction so that a sudden passage of a hard scybalous mass could be particularly difficult and traumatizing to it.
- Large haemorrhoids and hypertrophid anal papillae may cause fissure due to traction when these prolapsed at defecation.
- Enthusiastic use of ointments for variety of anal conditions causes thinning of skin of the anal canal thus predisposing to an easy tear.
- Sometimes trauma to anal canal caused by nozzle of enema, results in fissure .
Pathophysiology
An anal fissure is typically found in the posterior midline just within the anal verge. More than 98% of fissure in males and nearly 85% in females occur in this way. The superficial external anal sphincter arise from the tip and side of the coccyx and surrounds the anal canal leaving a weak area on the posterior wall this causes it to tear when it is over stretched during the passage of a hard stool. In addition, anal crypts are more marked posteriorly and which tends to harbor subclinical infection, which causes the epithelial lining to be friable. Anterior fissure in women (15%) is often due to trauma of parturition causing old tear to break down.
An acute fissure is an ulcer, the base of which is formed by longitudinal muscle fibers. When it become chronic, the deeper circular fibers of the internal sphincter are seen to form the floor of the fissure. The changes which develops in a chronic fissure are -
- Thickening of the edge of the ulcer.
- Development of an edematous tag of skin at its lower end (sentinel piles)
- Hypertrophy of the anal papilla at its upper end .
The sentinel piles develops due to combination of infection and oedema.
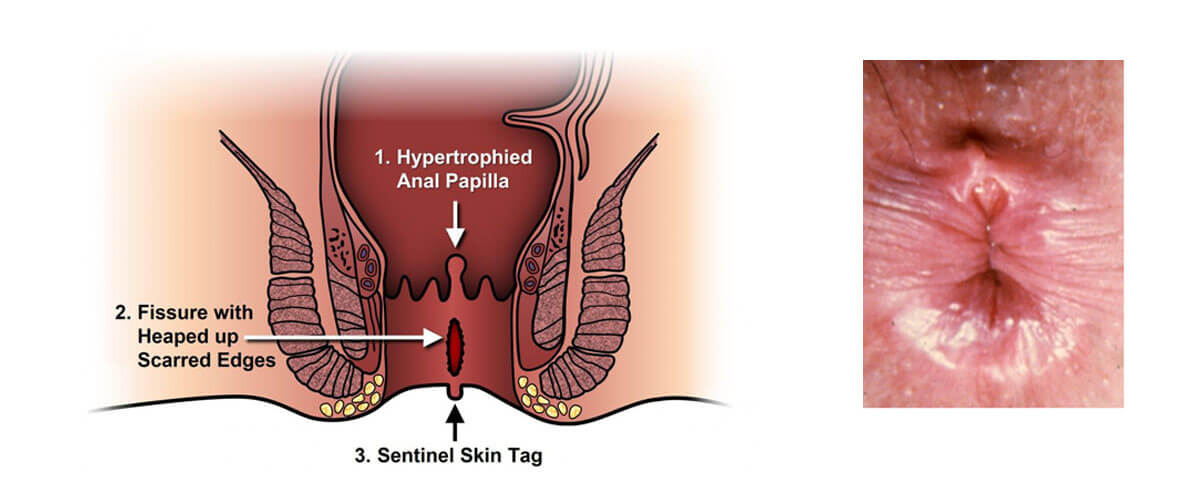
A chronic fissure thus has four typical features -
- A boat shaped ulcer with indurated edges.
- Fibers of internal sphincter forms the floor.
- A rounded swelling (hypertrophied anal papilla) at its upper end.
- A tag of skin at its lower end (sentinel piles).
Infection of the base may lead to an abscess, which may rupture through the base of the fissure or through the skin nearby leaving a short subcutaneous fistula.
An anal fissure situated away from the midline usually has a cause within the anal canal in the form of a fibrous polyp , large haemorrhoids or a hypertrophied anal papilla. If a cause is not found , such a fissure should immediately raise suspicion of another pathology ( example – tuberculosis, syphilis, leukemia, squamous cell carcinoma or inflammatory bowel disease especially Crohn’s disease. Fissure in inflammatory bowel disease tends to be multiple, broad and situated away from the midline. The spasm normally associated with a nonspecific fissure is minimal or abscent.The possibility of such fissure must be borne in mind since operative interference may cause delay in wound healing or an early recurrence.
Diagnosis
Pain of tearing, cutting or burning type associated with defecation and lasting for a variable period after defecation is the symptom. With the onset of suppuration the pain become throbbing in character and continuous. Each act of defecation become an agony due to fear of pain the act of defecation may be postponed leading to constipation. A vicious cycle of pain, constipation and pain is setup. Bleeding is seldom more than a few drops and is bright in color. Streaks of blood may be seen on the stool surface. In an acute fissure, reflex symptom of dysuria or pain radiating down the thighs is common. In chronic fissure , irritation and discharge which soils the underclothing are present . A swollen skin tag be felt outside the anus (sentinel piles).
Treatment
Many fissure heals spontaneously in two or three weeks. These are usually superficial lesion which have been attended by a short history. of pain. In contrast a chronic fissure are most resistant to any form of conservative treatment, though there may be temporary relief of symptoms, but the trouble tends to recur frequently. To save the patients unnecessary discomfort it is desirable to make an early decision as to whether a fissure is likely to heal under a conservative regimen or whether an operation will be required.
Features indicating chronicity and the need for operation – A long continuous or intermittent history of pain obviously suggests a chronic lesion is present. On examination the findings that indicate chronicity are a large sentinel tag of skin, indurations on the edge of the fissure and the exposure of the internal sphincter in the floor of the fissure. When these signs are present a lasting cure is unlikely to be achieved without operation. A recent fissure of a more superficial character, operative measure may sometime be required because of the pain which the patient is unwilling to tolerate any more or because of abscess or fistula formation.
The operative results of anal fissure are not always satisfactory. Various forms of complications like rectal incontinence, faecal soiling of under clothes and recurrences are common problems after operations for anal fissure. Majority of the patients are dissatisfied with modern operations.
Ayurvedic treatment of Anal Fissure
The treatment of Anal fissure consists of hot sitz bath twice daily morning and evening after defaecation. Medicated oil enema is given twice daily before defaecation and mild laxative like panchsakar choorn One T.S.F. at bed time is given to remove the constipation. In spite of these treatment if the pain is persistent in chronic, non healing, infected fissure Kshar Sutra ligation is done under local anesthesia. The results of Kshar sutra treatment in anal fissure is excellent with high success rate of 98.0% . The post operative complications are nil. 350 cases of chronic non healing anal fissure have been treated by Kshar Sutra at this centre with excellent cure rate.
Fatty, fast and fried food are avoided, soft palatable light and high fibrous diet is recommended. Two wheeler vehicles, scooter, Motor Cycle, Cycle are avoided because these vehicles aggravate the anal fissure.
